ML4HF™ synthesizes complex invasive hemodynamic data into clear classifications, predicted trajectories, and referral-ready clinical snapshots — so every clinician at the bedside or in the cath lab can act earlier, with confidence.
The full workflow — from focused entry to a referral-ready snapshot — on the device that's already in your white coat.
Modern cardiac catheterization produces dense, sophisticated hemodynamic data — pressure-volume mechanics, energetic reserve, ventricular-arterial coupling. Most of it goes unused because most clinicians don't have time to compute it by hand.
So patients get staged on what's quick: blood pressure, cardiac output, filling pressures. The nuance — and the earlier referral that nuance enables — gets lost.
ML4HF™ closes that gap. It does the hard math behind the scenes and returns the answer in the language clinicians already use, in time for it to change the decision.
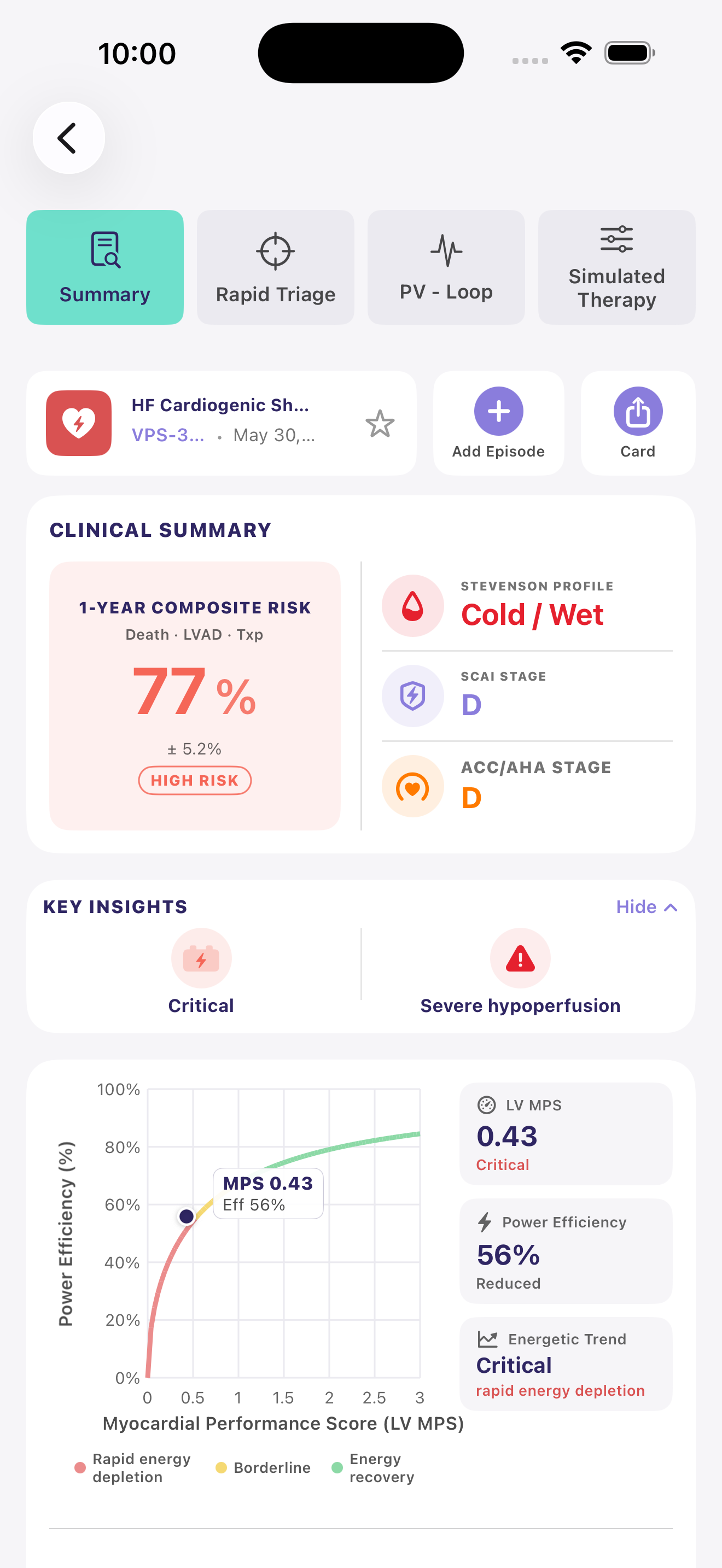
Pressure-volume mechanics, energetic reserve, ventricular-arterial coupling — computed in the background, returned in the staging language clinicians already use.
From the values you already have at the bedside or in the cath lab. No new monitoring. No extra steps.
Trained on thousands of advanced HF cases. Refined continuously with every de-identified case clinicians contribute.
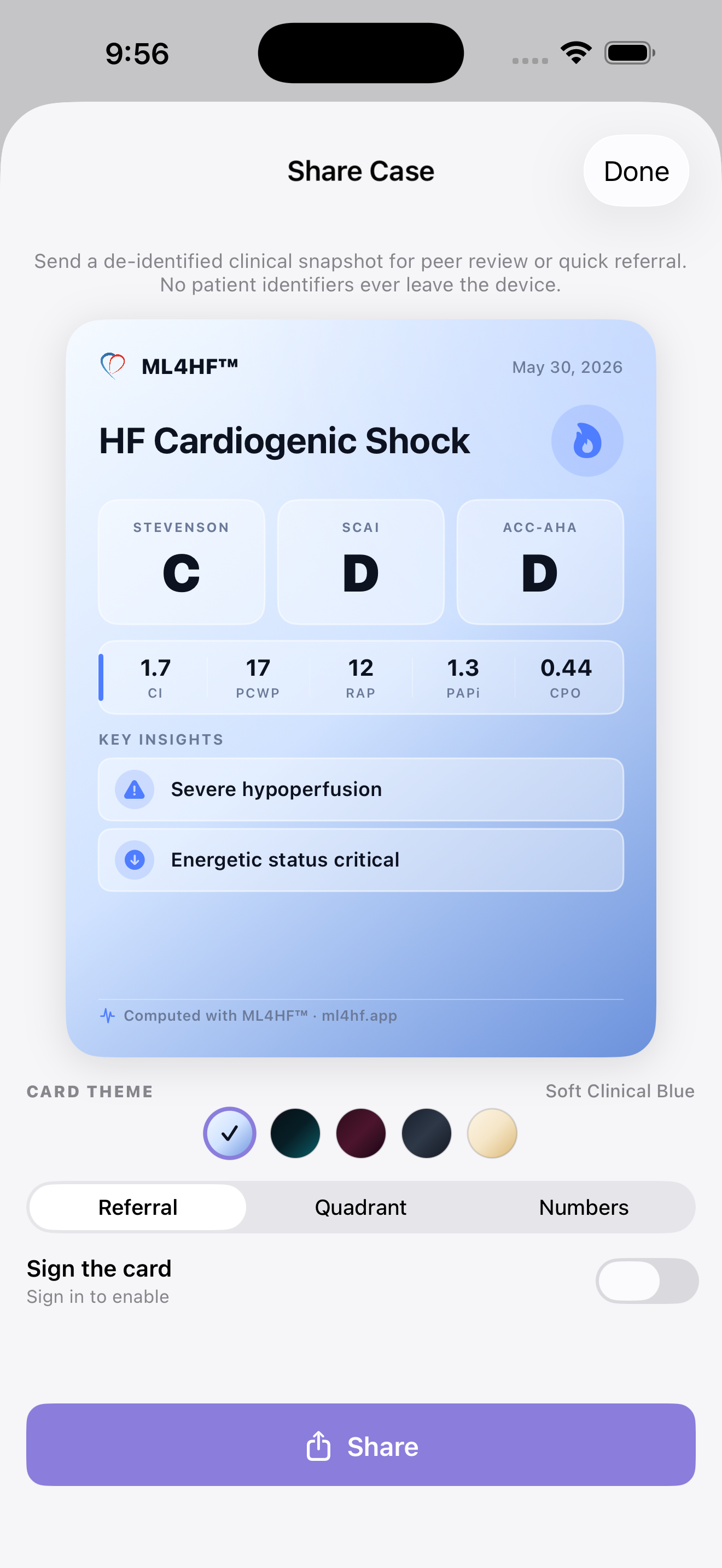
Energetic indices move before classical staging catches decline. Refer when it still matters — with a snapshot the receiving team can act on.
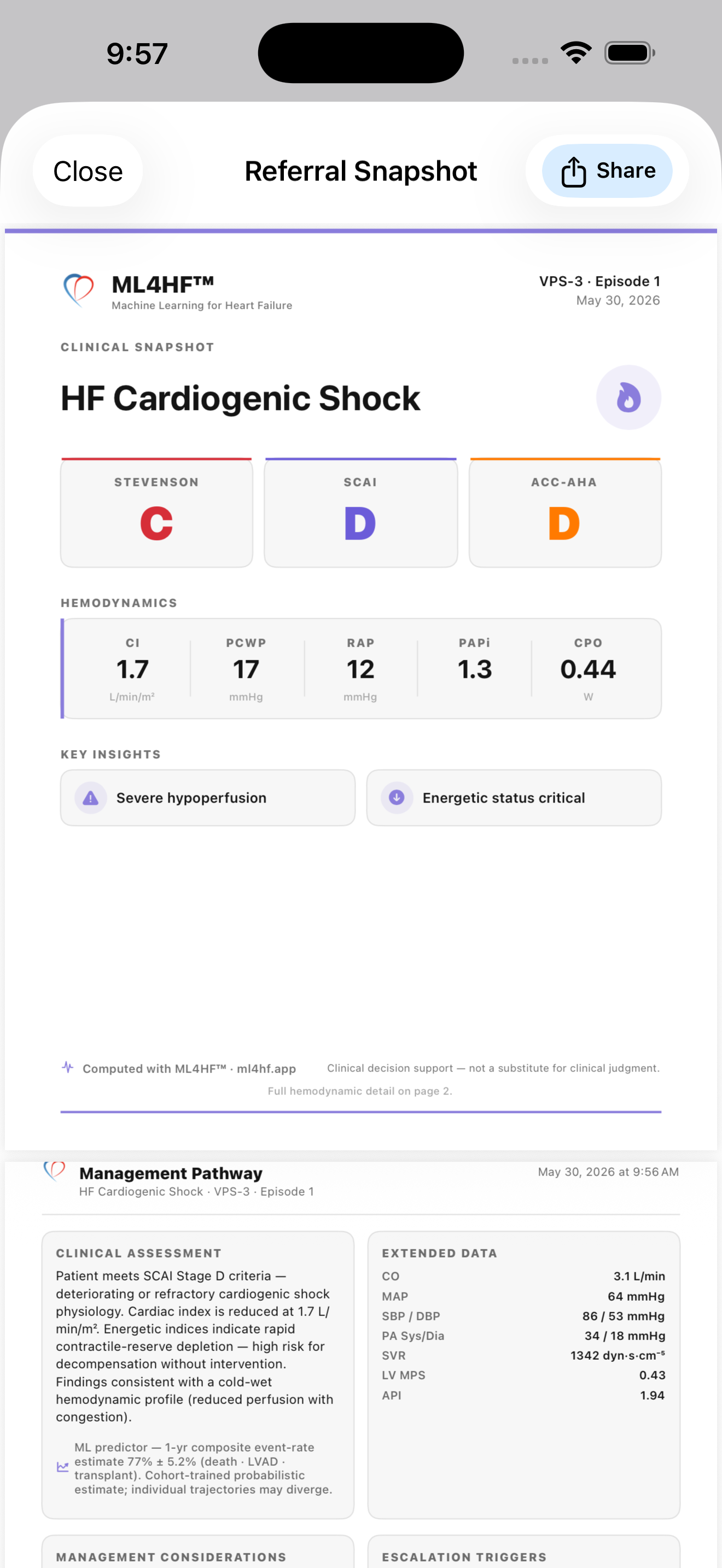
Enter the values you already have. ML4HF™ reconstructs the patient-specific pressure-volume loop, computes the full panel of energetic indices, renders Stevenson, SCAI, and ACC/AHA staging — and pairs them with a phenotype-driven management pathway — in a single screen.
ML4HF™'s predictive engine is trained on a large cohort of patients with advanced and end-stage heart failure — the population in which accurate trajectory information is the difference between timely referral and a missed window. The model learns continuously from every de-identified case clinicians contribute, so accuracy refines in step with the field.
Most cardiogenic shock and end-stage HF patients arrive at advanced HF programs later than the data supports — sometimes by days, sometimes by weeks. The cost is measurable in mortality, LVAD eligibility, and transplant candidacy.
Energetic indices — contractile reserve, ventricular-arterial coupling, pulmonary arterial pulsatility — move before classical staging captures decline. ML4HF™ surfaces those changes the moment your hemodynamic data is in.
And when it's time to refer, the receiving team gets a phenotype, a trajectory, and a management pathway — not a fax. Less back-and-forth, less time lost, more options preserved.
When your fellows, attendings, and APPs all use ML4HF™, every case is computed the same way, attributed correctly, and surfaced to the team in a shared library. The phenotype-driven referral pathway makes intake faster and decision-making more consistent across the program.
A two-stage pipeline: a patient-specific pressure-volume reconstruction that yields the energetic indices, then an ML predictor trained on annotated advanced-HF outcomes that returns a 1-year composite event-rate estimate with an uncertainty band. The receiving clinician sees both the synthesis and the underlying physiology — never a black box.
ML4HF™ is built by the clinicians who work between bedside hemodynamics and the decisions that follow. The advanced cardiovascular physiology under the hood — pressure-volume mechanics, energetic reserve, trajectory modeling — exists because we needed it ourselves. Every feature serves a single goal: getting the right patient to the right program earlier, with better information in hand.
Early access invites are rolling out by specialty. Tell us who you are and we'll be in touch with a TestFlight link.